
Why Medicine Pretends Precision While Delivering Approximation
Modern medicine speaks the language of precision.
Milligrams.
Concentrations.
Standard doses.
Everything appears exact.
A tablet contains 500 mg.
Not 499. Not 501.
It feels scientific. Controlled. Reliable.
But this precision exists in only one place:
The pill.
Not the patient.
1. Where Precision Begins—and Ends
Inside a tablet or capsule, dosing is exact.
Manufactured to tight tolerances.
Validated. Reproducible.
But the moment that pill enters the body:
- It disintegrates unpredictably
- It dissolves variably
- It is absorbed inconsistently
And the illusion begins to break.
Precision in manufacturing becomes approximation in biology.
2. The Myth of “One Dose Fits All”
The system assumes:
A single fixed dose can serve millions of people
But humans are not uniform.
We differ in:
- Body weight
- Enzyme activity
- Organ function
- Genetics
- Disease state
A 500 mg dose in one person may be:
- Insufficient
- Optimal
- Excessive
There is no universal truth.
Only averages.
3. The Pharmacokinetic Reality
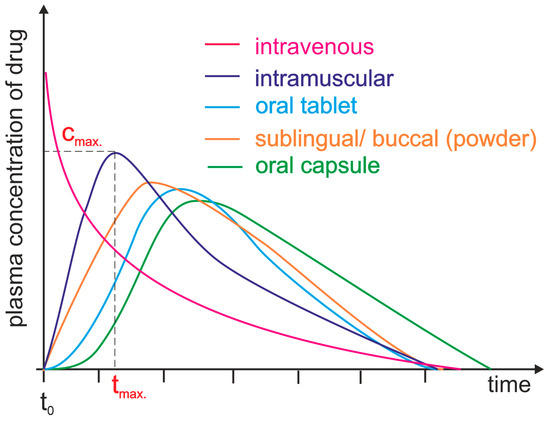
In pharmacokinetics, this is well understood.
Give the same dose to different patients, and you see:
- Different peak concentrations
- Different times to effect
- Different durations of action
The curves diverge.
Sometimes slightly.
Sometimes dramatically.
And yet, the dose remains the same.
4. Discrete Units vs Continuous Biology
Tablets and capsules force medicine into:
- 200 mg
- 400 mg
- 500 mg
Discrete steps.
But biology doesn’t operate in steps.
It operates on a spectrum.
There is no inherent reason why:
Your optimal dose = exactly 500 mg
It might be:
- 347 mg
- 612 mg
- 428 mg
But those options don’t exist.
Because the system cannot easily deliver them.
5. The Workarounds We Accept
To bridge this gap, we improvise:
- Split tablets
- Adjust frequency
- Combine strengths
But these are not solutions.
They are approximations layered onto approximations.
Each introduces:
- Variability
- Complexity
- Error
We simulate precision—without achieving it.
6. When Approximation Becomes Risk
For some drugs, this variability is manageable.
For others, it is critical.
Small differences in exposure can mean:
- Reduced efficacy
- Increased side effects
- Toxicity
And yet, the system still relies on:
Fixed, standardised doses
Because changing the format is harder than accepting the error.
7. The Economics of Simplicity
Why does this persist?
Because fixed dosing enables:
- Mass manufacturing
- Simplified regulation
- Global scalability
It reduces complexity—for the system.
Even if it introduces variability—for the patient.
8. The Psychological Comfort of Numbers
There is another reason the illusion persists:
Numbers feel precise.
500 mg feels exact.
Scientific. Trustworthy.
Even if the biological outcome is not.
The number reassures us—
even when reality is uncertain.
9. The Ibumix Perspective
The fixed-dose model is not wrong.
It is incomplete.
It was designed for a world where:
- Manufacturing was the constraint
- Simplicity was essential
But today, the constraint is different:
Biological variability
And the system has not caught up.
10. A Different Model of Precision
True precision medicine would mean:
- Dose tailored to the individual
- Delivery adjusted dynamically
- Exposure controlled, not assumed
Not:
- Fixed units
- Static formats
- Approximate outcomes
But real, measurable alignment between:
- What is given
- And what is received
11. The End of the Illusion
The fixed dose is not precision.
It is a simplification that worked at scale.
But scale is no longer the only goal.
Now, the goal is:
- Accuracy
- Personalisation
- Performance
And that requires rethinking the foundation.
Final Line
The pill delivers an exact number.
The body receives an approximation.
That gap is where the future of medicine will be built.
Part of the Ibumix series on the tablet’s limits. Start with the overview: Why the tablet is pharma’s bottleneck.